Brief Context
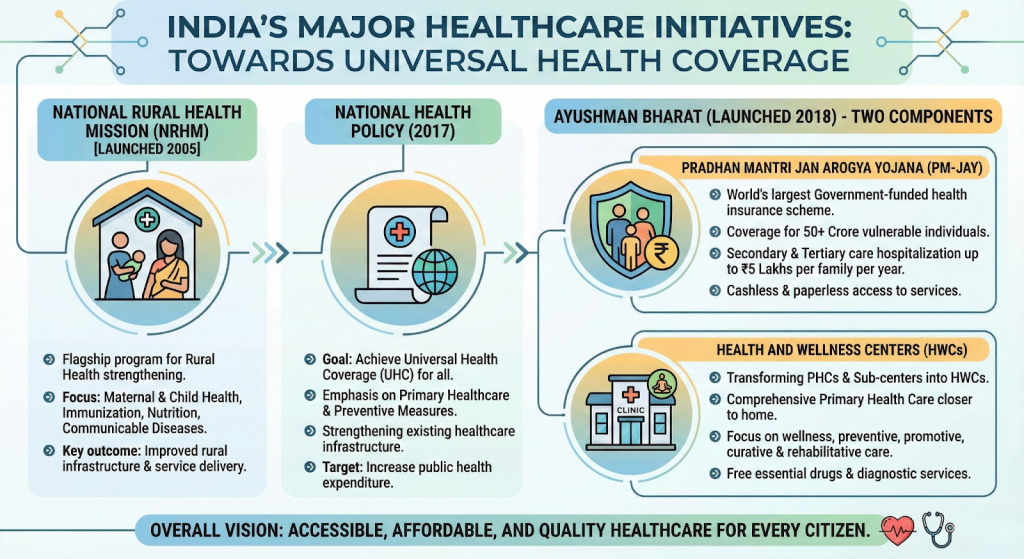
Published on: 16th December, 2025 India committed to Universal Health Coverage (UHC) through the National Health Policy (NHP), 2017 and SDG-3, operationalised mainly via Ayushman Bharat (AB).
Source Content
Syllabus: GS2/Health/GS3/Economy
Context
- India committed to Universal Health Coverage (UHC) through the National Health Policy (NHP), 2017 and SDG-3, operationalised mainly via Ayushman Bharat (AB).
- Despite progress, India continues to face a serious access–affordability–quality gap, indicating that UHC goals remain underachieved.
What is Universal Health Coverage?
- It means that all people have access to the full range of quality health services without financial hardship.
- Key components of UHC include:
- Access to Care: Everyone should be able to obtain necessary health services when they need them.
- Quality Services: The care provided should be effective, safe, and of good quality.
- Financial Protection: Individuals should not face financial difficulties due to medical expenses.
- UHC is rooted in the universal human right to health, affirmed in international covenants and the Alma-Ata Declaration (1978), which prioritised comprehensive primary healthcare.
Need For Universal Health Coverage in Indian Context
- Historical Commitment to Universal Healthcare:
- Bhore Committee (1943–46) reflected a clear preference for universal healthcare over insurance-based UHC.
- Policy Evolution after Independence:
- India’s National Health Policy of 1983 recognized the goal of “Health for All” and emphasized the importance of primary healthcare and equitable distribution of healthcare resources.
- Shift towards Insurance-led UHC:
- Welfare Schemes like Rashtriya Swasthya Bima Yojana (RSBY) 2008 and Ayushman Bharat–PMJAY institutionalised UHC but reinforced an insurance-heavy approach.
- Weak Public Health System and Rising Private Dependence:
- Chronic underfinancing of primary healthcare has led to poor quality public provisioning, shortage of infrastructure and workforce.
- National Sample Survey (NSS) data show growing reliance of the poor on private healthcare, rising out-of-pocket expenditure (OOPE) & increased household indebtedness.
- Constitutional Basis for UHC:
- The Directive Principles of State Policy in Part IV of the Constitution provides a basis for the right to health.
- Article 39 (e) directs the state to secure the health of workers; Article 42 emphasises just and humane conditions of work and maternity relief; and Article 47 casts a duty on the state to raise the nutrition levels and standard of living, and to improve public health.
- The Constitution also endows the panchayats and municipalities to strengthen public health under Article 243G.
- Post-Covid Realisation:
- The Covid-19 pandemic exposed inequities in insurance-based access, exclusion of informal workers and migrants & fragility of hospital-centric models.
- Present Policy Direction:
- Currently, India aims to attain UHC through the expansion of the Ayushman Bharat-Pradhan Mantri Jan Arogya Yojana (AB-PMJAY), the flagship publicly financed health insurance (PFHI) scheme of the Union government.
Challenges in Adopting UHC in India
- Resource Constraints: India faces significant funding limitations in healthcare, with a low public health expenditure compared to many other countries. This affects the ability to provide comprehensive services.
- Low public health expenditure (~2.1% of GDP), below the NHP target of 2.5%.
- Infrastructure Gaps: Many areas, especially rural regions, lack adequate healthcare infrastructure, including hospitals, clinics, and trained personnel, making access to care difficult.
- Healthcare Workforce Shortages: There is a shortage of healthcare professionals, particularly in rural areas, leading to disparities in access and quality of care.
- Fragmented Health Systems: India’s healthcare system is a mix of public and private providers, leading to inconsistencies in quality and accessibility.
- And, Health is a State subject, while financing and flagship schemes are centrally driven, leading to uneven outcomes.
| Lessons from Global Experience
– WHO Alma-Ata Declaration (1978) emphasised primary healthcare as the foundation of UHC. |
Making Ayushman Bharat 2.0 More Effective
- Shift from Coverage to Care: Move from hospitalisation-centric insurance to universal healthcare.
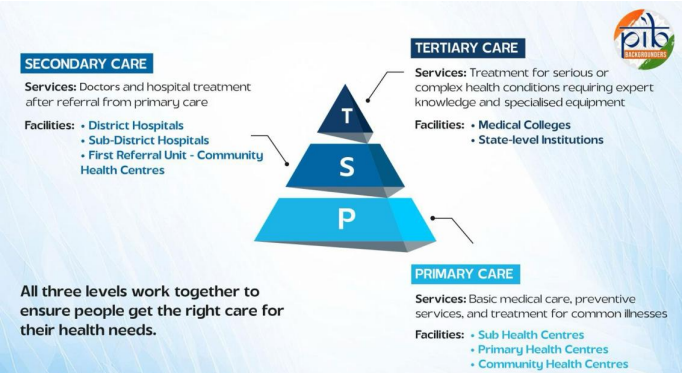
- Strengthen comprehensive primary healthcare as the first point of contact.
- Strengthen Primary and Secondary Care: Invest in infrastructure, diagnostics, medicines and referral systems.
- Use HWCs as gatekeepers to reduce avoidable hospitalisation.
- Increase Public Investment: Raise health spending to at least 2.5% of GDP.
- Prioritise preventive and promotive care and social determinants of health.
- Digital and Human Resource Reforms: Integrate ABHA ID, interoperable health records and disease surveillance.
- Address workforce shortages through task-shifting, local recruitment and continuous training.
- Better Regulation and Strategic Purchasing: Standard treatment guidelines, cost controls and accountability mechanisms.
- Align insurance schemes within a strong public health system, as seen globally.
| Daily Mains Practice Question [Q] Financial protection without strong public health provisioning can deepen healthcare inequities. Examine |
Source: IE